How much does an electronic medical record system cost?
Two pricing models cover the vast majority of EMR deployments:
SaaS subscription: $200 to $1,200 per provider per month, or $600 to $1,200 per user per year. This covers software access, hosting, automatic updates, and basic support. Most cloud-based EMR products for small practices sit in the $200-$500/month range for a solo or small group practice.
Custom or hybrid build: $50,000 to $150,000 upfront for most small-to-mid size clinic projects. This covers requirements analysis, development, data migration, training, and deployment. Projects with complex specialty workflows or local compliance requirements (PhilHealth, PDPA, Vietnam MOH) run higher.
A useful shortcut: if you are a solo practitioner or a clinic with under 10 providers and standard workflows, a SaaS product is almost certainly the right starting point. If your workflows differ significantly from standard primary care, or if local compliance requirements are complex, a custom or hybrid build is worth evaluating seriously.
EMR price breakdown: What you are actually paying for
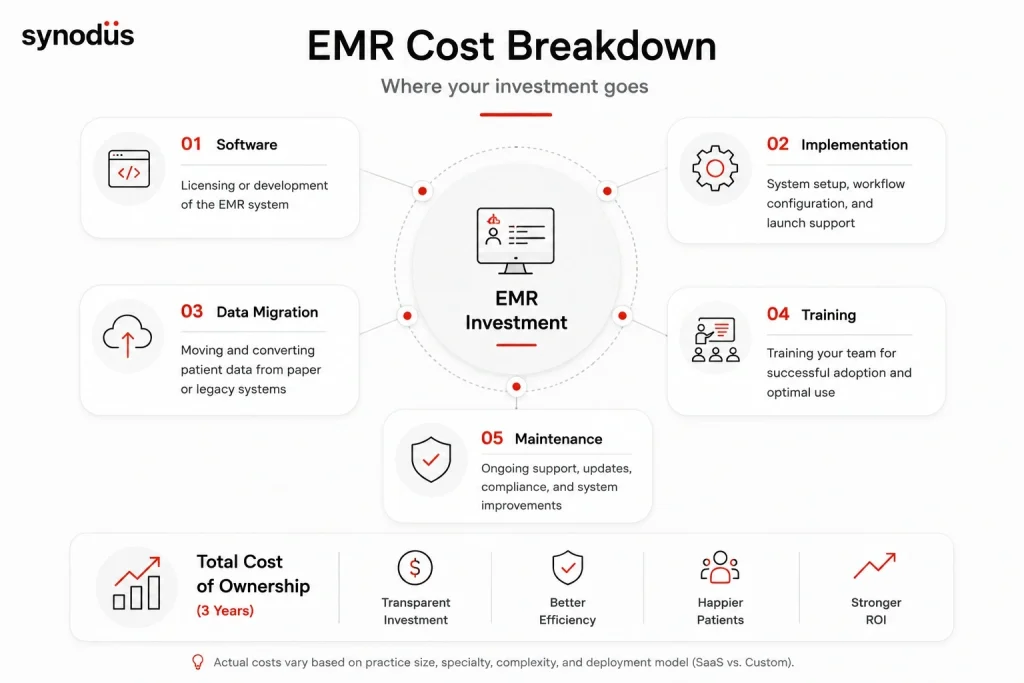
Software licensing or development
For SaaS products, this is the monthly or annual subscription fee. Watch for:
- Per-provider vs per-user pricing (a clinic with 3 doctors and 10 support staff pays very differently depending on which model applies)
- Module-based pricing where core EMR is cheap but billing, patient portal, and e-prescribing are add-ons
- Annual vs monthly billing (annual typically saves 10-20%)
For custom builds, the development fee covers the team building your system: project manager, frontend and backend developers, UX designer, QA, and business analyst. Hourly rates vary significantly by region:
| Region | Hourly rate |
|---|---|
| US, Australia, Western Europe | $80-$200/hr |
| Eastern Europe | $40-$80/hr |
| Vietnam, India, Malaysia | $20-$50/hr |
Rate differences do not always reflect quality differences. Many APAC vendors with healthcare-specific experience deliver comparable output at 40-60% of US rates.
Implementation and setup
SaaS products typically charge a one-time setup fee covering system configuration, workflow mapping, and initial training. For small practices, this ranges from $1,000 to $15,000 depending on complexity.
Custom builds fold implementation into the project cost. Implementation support for US-based projects averages around $6,200 per user according to a 2025 analysis. For a 10-provider clinic, that is $62,000 in implementation costs before the software fee.
Data migration
Moving patient records from paper or a legacy system is consistently the most underestimated cost in EMR projects.
- Paper to digital: scanning, indexing, and data entry add up quickly at scale. A clinic with 5,000 active patients and 10 years of paper records is looking at weeks of migration work.
- Legacy system to new EMR: depends heavily on whether the legacy system can export in a standard format. Proprietary formats require custom extraction scripts. Budget $50-$200 per patient record for complex migrations in the US market; lower with offshore resources.
- Run a data audit before getting any vendor quotes. Knowing your exact data volume and format prevents surprises mid-project.
Training
Training costs scale with practice size and system complexity. Budget for:
- Initial role-based training before go-live (clinical staff, front desk, billing)
- Reinforcement training 2-4 weeks post go-live – this is when real usage gaps surface
- Ongoing training for new hires
Practices that underinvest in training consistently report lower adoption and slower ROI. The training cost is real, but the cost of low adoption is higher.
Ongoing maintenance
For SaaS: included in the subscription. Watch for price increases at renewal – annual increases of 5-15% are common in healthcare SaaS contracts.
For custom builds: budget 15-20% of the original build cost per year for maintenance, security patches, regulatory compliance updates, and feature additions. This is ongoing, not optional.
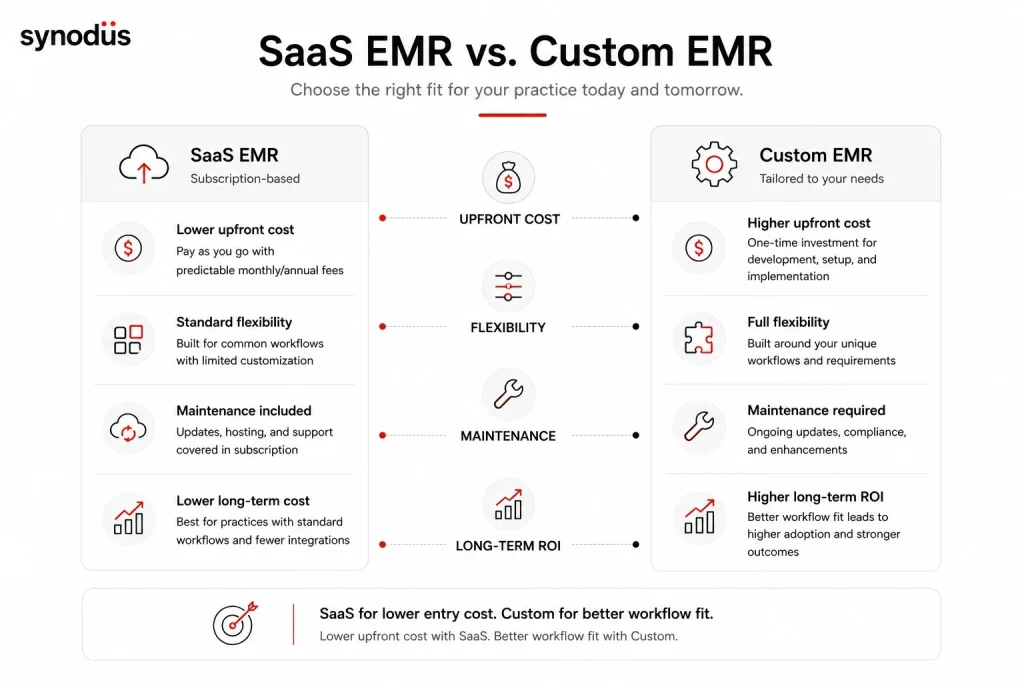
Total cost of ownership: SaaS vs custom over 3 years
For a 5-provider primary care clinic as an example:
| Cost component | SaaS ($400/provider/month) | Custom build |
|---|---|---|
| Software (year 1) | $24,000 | $80,000 (build cost) |
| Implementation/setup | $5,000 | Included |
| Data migration | $2,000 | $2,000 |
| Training | $3,000 | $3,000 |
| Year 2 software | $24,000 | $12,000 (maintenance) |
| Year 3 software | $25,200 (5% increase) | $12,000 |
| 3-year total | ~$83,000 | ~$109,000 |
The custom build costs more at year 1 but produces a system built around your workflows – which typically delivers better adoption and faster ROI. By year 5, the gap narrows further as SaaS annual increases compound.
This comparison assumes a straightforward SaaS implementation. Complex specialty workflows or compliance customization on a SaaS platform can add $20,000-$50,000 in consulting fees, shifting the comparison.
What drives EMR cost up
Specialty workflows. Standard primary care EMR products are priced for standard workflows. Mental health (treatment plan requirements, different note formats), oncology (protocol tracking, chemotherapy order sets), and ophthalmology (integrated imaging) all require either a specialty-specific product or significant customization – both of which cost more.
Local compliance requirements. For clinics in Southeast Asia, Middle East, or other markets with specific regulatory environments, getting an EMR to comply with local standards requires development work that standard OTS products do not include. PhilHealth eClaims 3.0 certification, Vietnam BHYT integration, and Malaysian PDPA compliance are not built into Epic or Athenahealth.
Integration scope. Each external system your EMR needs to connect with – lab equipment, imaging, insurance portals, pharmacy systems – adds integration cost. A clinic that refers heavily to external labs and specialists has a fundamentally more complex integration requirement than a self-contained practice.
Number of locations. A single-location clinic has straightforward infrastructure. A multi-location group adds network infrastructure, centralized data management, and more complex user access configuration.
What drives EMR cost down
Cloud deployment. Eliminates server hardware, infrastructure maintenance, and the IT staff to manage it. For small practices without a dedicated IT team, this is the primary cost advantage of SaaS.
Standardized workflows. The closer your clinical workflows are to what a standard OTS product expects, the less customization you need. Practices that are willing to adapt their processes to the software pay less than those that require the software to match their processes exactly.
Phased implementation. Starting with core modules (clinical documentation, e-prescribing, basic scheduling) and adding patient portal, advanced analytics, and specialty modules in later phases spreads cost over time and reduces upfront risk.
Outsourcing to lower-cost regions. For custom builds, development teams in Vietnam, India, or Eastern Europe deliver comparable healthcare software quality at 40-60% of US rates. The key is verifying healthcare-specific experience, not just general development capability.
Open-source foundations. Using OpenEMR or OpenMRS as a starting point eliminates licensing fees and can significantly reduce build cost for practices with technical capacity to support it.
ROI timeline for small practices
Research puts the average payback period for solo and small practices at 2.5 years. Primary care practices average approximately 10 months. The variation is explained primarily by billing volume – practices with higher patient throughput see faster revenue cycle improvement.
The main ROI drivers for small practices:
Billing accuracy: Automated charge capture and coding assistance reduce missed charges and claim denials. A practice with a 10% denial rate that improves to 5% through EMR automation sees direct revenue impact within 6-12 months.
Administrative time reduction: Research found savings of approximately 75 minutes per provider per day once staff fully adapted to the system. For a solo practitioner billing at $200/hour, that is $25,000/year in recovered productive time.
Paper and storage elimination: Printing, filing, and physical storage costs are ongoing and easy to underestimate at scale. Most practices see $5,000-$15,000/year in savings here.
Reduced transcription costs: Practices that previously used transcription services typically eliminate or significantly reduce this expense after EMR adoption.
For a full breakdown of what benefits to expect and what limitations to plan for, see the EMR advantages and disadvantages guide.
Hidden costs most vendor quotes exclude

Productivity loss during transition. Most practices experience a 10-20% productivity dip for 4-8 weeks after go-live as staff adapt. For a 5-provider clinic, that is real revenue impact. Plan for it, do not be surprised by it.
Compliance updates. Regulatory requirements change. ICD-11 is rolling out. Local MOH standards update. New payer requirements emerge. For SaaS products, major compliance updates may be included – or may be charged as upgrades. For custom builds, budget for compliance maintenance annually.
Contract renewal price increases. Healthcare SaaS contracts commonly include automatic renewal with 5-15% annual price increases after year 1. Verify the renewal terms before signing, not after.
Data migration complexity discovery. Practices that skip the data audit before getting vendor quotes frequently discover mid-project that their legacy data is messier or more voluminous than expected. Run the audit first.
Interface development for lab and imaging. Many vendor quotes assume you will enter lab orders manually. If you want bidirectional electronic integration with your reference lab, that is a separate project with a separate cost.
Build your EMR with Synodus
If your practice has specific workflow requirements, local compliance needs, or integration complexity that standard OTS products do not handle well, a custom or hybrid build is worth a serious look.
Synodus is a Vietnam-based healthcare software development company with 250+ developers and 30+ healthcare implementations across APAC. Their hybrid model starts from a validated EMR base and extends it with custom modules, local compliance layers, and integrations – delivering the workflow fit of a custom build at lower cost than starting from scratch.
Multi-field hospital complex – 700 beds, 2,500 outpatients and 800 staff daily. Custom EMR with cloud-based records, two-layer encryption, e-prescription, document scanning, and full integration with HIS, scheduling, and inventory. Built in 4 months. Results: 70% improvement in operational efficiency, 90% decrease in incident rates, 3x faster diagnosis, 85% of documents digitalized. Read the full EMR/EHR case study.
Development rates start at $25/hour. Projects start within 48 hours of scoping completion
FAQs
Cloud-based SaaS EMR products for small practices typically run $200-$500 per provider per month. A 3-provider clinic can expect $600-$1,500/month in software fees, plus a one-time setup fee of $1,000-$15,000. Custom builds for small practices start around $50,000.
Yes. OpenEMR and OpenMRS are open-source EMR systems with no licensing fees. Implementation, hosting, training, and maintenance costs still apply. For small clinics with technical capacity or access to a developer, total cost can be significantly lower than commercial alternatives. See the free and open source HIS software guide for a detailed comparison of open-source options.
EMR systems serve a single practice and typically involve less integration complexity – lab, imaging, and billing within the practice. EHR systems extend to cross-provider data sharing and population health functions, which adds interoperability development and compliance costs. EHR implementations that require full cross-provider integration typically cost 20-40% more than standalone EMR deployments of equivalent scale. For a full comparison of what EMR, EHR, and PHR actually are, see the EMR vs EHR vs PHR guide. For a full EHR cost breakdown, see the EHR cost and ROI guide.
SaaS products: $600-$1,200 per user per year at the low-to-mid market. Enterprise-tier products (Epic, Oracle Health) operate on custom enterprise pricing. For a 10-provider clinic on a mid-market SaaS product, expect $60,000-$120,000/year in software fees alone, before implementation, training, and maintenance.
Yes, significantly. Development teams in Vietnam, India, and Eastern Europe deliver comparable healthcare software at 40-60% of US rates. The critical factor is healthcare-specific experience – verify the vendor has built and deployed clinical systems before, not just general software. For guidance on what to look for in a vendor, see the hospital information system companies guide.
Solo and small practices: 2.5 years on average. Primary care practices: approximately 10 months. The timeline is driven primarily by billing improvement – practices with higher denial rates see faster financial return. Most practices see measurable billing improvement within 6-12 months of full adoption, even if full payback takes longer





