Quick reference: EMR pros and cons
| Advantage | Disadvantage |
|---|---|
| 30-38% reduction in medication errors | High upfront implementation cost |
| 75 min/provider/day saved (post-adaptation) | Productivity dip during transition (4-8 weeks) |
| Instant record retrieval vs. minutes to hours | Alert fatigue from poorly configured CDS |
| Automated billing reduces claim denials | Security risk: single point of breach |
| Preventive care rates up 10-20% | Vendor lock-in and data portability risk |
| Supports population health analytics | “Pajama time” – after-hours documentation burden |
| Audit trail automatic and complete | Interoperability gaps between systems |
| Eliminates storage and printing costs | Ongoing maintenance and upgrade costs |
Advantages of electronic medical records
1. Significant reduction in medication errors
The most consistently documented advantage of EMR adoption is its impact on medication safety. Clinical decision support systems built into EMR platforms provide real-time drug interaction checking, allergy alerts, and dosing guidance at the point of prescribing, catching errors before they reach patients.
The research is specific: a 2023 study published in npj Digital Medicine tracked a hospital’s transition from paper to fully digital records and found a 38% reduction in voluntarily reported medication incidents, with prescribing errors falling from 52.8% to 15.7% of orders reviewed. A separate Carnegie Mellon analysis linked full EMR adoption to approximately a 30% reduction in prescription errors. For a real-world example of these gains in an APAC hospital, see the EMR/EHR case study for a multi-field hospital complex.
For patients with complex medication regimens, allergies, or multiple prescribers, this is the single most important clinical benefit of EMR adoption.
2. Time savings for clinical staff – with an important caveat
Research published in PubMed Central found savings of approximately 75 minutes per provider per day once clinical staff fully adapted to an EMR system. That time returns directly to patient care.
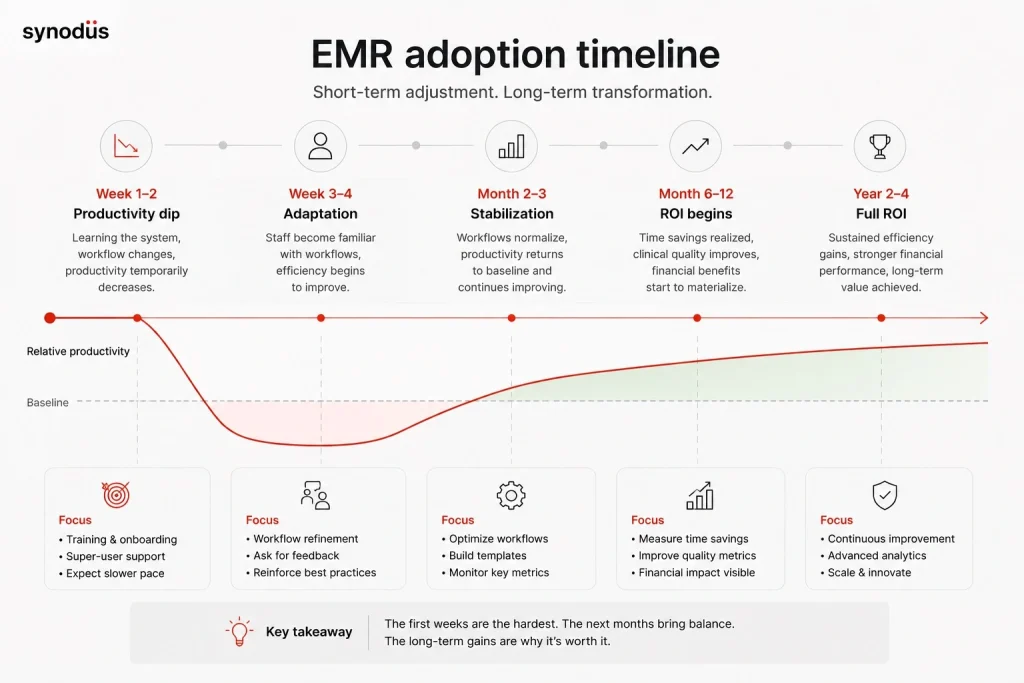
The caveat matters: this gain comes after adaptation, not immediately. Small practices often experience short-term issues like temporary loss of productivity during implementation, with most organizations seeing a 10-20% productivity dip in the first 4-8 weeks. Planning for this transition period is as important as the long-term benefit it leads to.
Cloud-based EMRs let healthcare professionals update charts and review histories in real-time, boosting collaboration and continuity of care – particularly valuable in multi-provider practices where staff need access to current patient data from different locations or devices.
3. Faster and more reliable record access
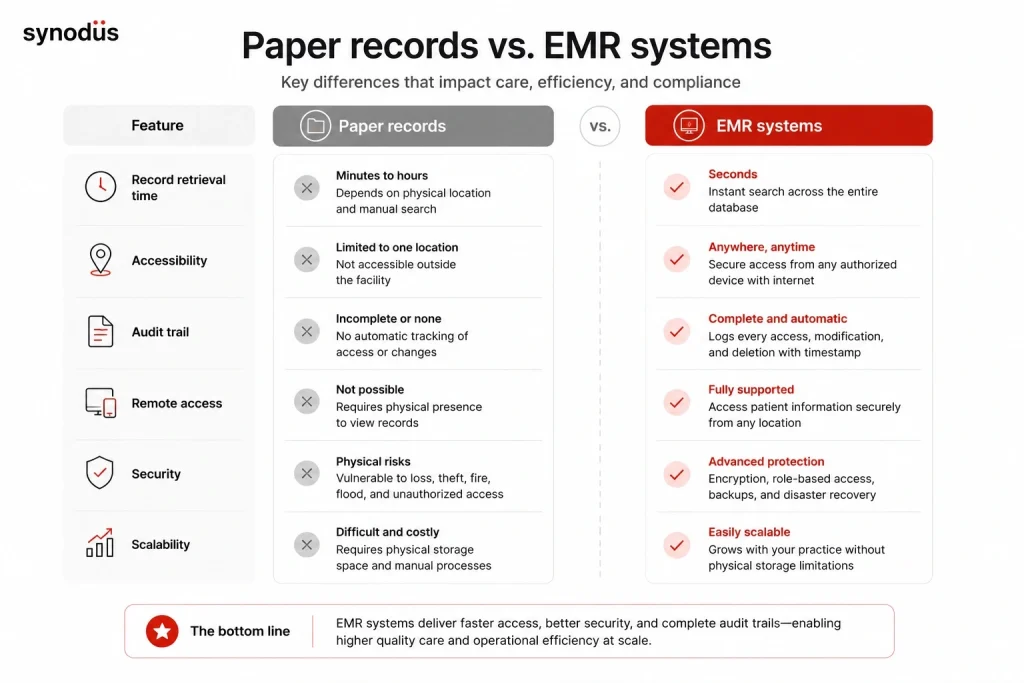
Paper records take minutes to hours to retrieve. EMRs return results in seconds. In emergency settings, where a patient’s allergy list or current medications need to be confirmed immediately, this speed difference has direct clinical consequences.
Remote access is an extension of this: a physician can review a patient’s history from a different facility, consult on a case from home, or check recent lab results before a telemedicine appointment – none of which are practical with paper.
4. Improved preventive care and chronic disease management
EMR alerts and reminders raise screening and vaccination rates by 10-20% compared to paper-based systems. For chronic disease management – diabetes, hypertension, COPD – the ability to track trends across visits, set automated follow-up reminders, and identify patients overdue for monitoring is genuinely difficult to replicate in paper systems.
Population health tools built into modern EMRs allow practices to identify all diabetic patients with HbA1c above a threshold, all patients overdue for colorectal cancer screening, or all hypertensive patients not at blood pressure goal – enabling proactive outreach that paper systems cannot support at scale.
5. Revenue cycle improvement
Automated charge capture connects clinical documentation to billing in real time, reducing missed charges. Coding assistance suggests appropriate E&M codes based on documented complexity. Electronic claim submission with pre-submission error checking reduces denial rates.
Most practices see steady financial improvement within 12-18 months of full adoption. The initial period, however, often involves higher denial rates as staff learn new documentation requirements – which is a disadvantage discussed below.
6. Audit trail and compliance
Every access, modification, and deletion in an EMR is automatically logged with timestamp and user identifier. For HIPAA compliance, legal proceedings, or quality audits, this completeness is not achievable with paper records. Regulatory bodies and accreditation organizations increasingly expect this level of documentation integrity.
7. Research and population health data
EMRs are increasingly integral to clinical research, offering enhanced data accuracy, efficient participant recruitment, and seamless integration of real-world data. For academic medical centers and research-active practices, the ability to query structured EMR data across large patient populations enables research that would be impractical with paper charts.
Disadvantages of electronic medical records

1. High implementation cost – particularly for small practices
It is a major financial investment to transition from paper-based processes to a digital system, particularly for smaller organizations. Those small practices often experience short-term financial issues like implementation costs, the costs associated with ongoing maintenance, and a loss of revenue associated with the temporary loss of productivity during implementation.
One study projected that the total cost for a 280-bed acute care hospital going through a 7-year EHR installation was $19 million when all these factors were considered.
For smaller practices, cloud-based SaaS products reduce upfront costs significantly – typically $200-$1,200 per provider per month – but the five-year total cost of ownership including implementation, training, and ongoing support can still run into tens of thousands of dollars.
2. Productivity loss during transition
The transition from paper to digital is not seamless. Most practices experience a measurable productivity dip during implementation and the adaptation period immediately following go-live. Studies report that EHR implementation increased administrative workload, reducing time available for direct patient care during the transition period.
For small practices with limited staffing, even a temporary reduction in patient throughput has real financial consequences. The key mitigation is planning: role-based training before go-live, phased implementation where possible, and intensive on-site support in the first 4-8 weeks after launch.
3. Alert fatigue undermines clinical decision support
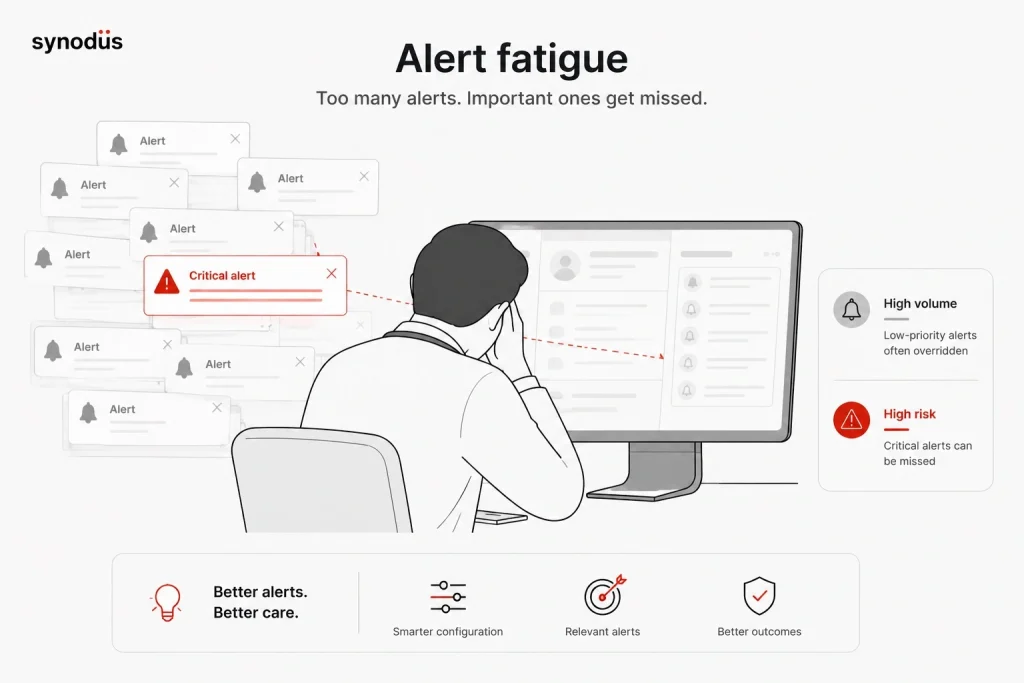
Clinical decision support is one of the most cited advantages of EMR systems – and one of the most commonly broken in practice. A study published in JAMIA found that 93% of drug interaction alerts were overridden in a large teaching hospital. A separate study found the acceptance rate for the most severe alerts fell from 100% to 8.4% after switching to a commercial EHR that generated six times more alerts.
When alert volume is too high or alert relevance too low, clinicians begin clicking through alerts reflexively. The clinical decision support system designed to catch errors becomes noise that gets ignored – including the genuinely important alerts.
This is a configuration problem, not an inherent EMR problem. Systems with properly configured alert thresholds, regularly reviewed and calibrated based on override patterns, deliver real clinical value. Systems deployed with default settings and never tuned do not.
4. Documentation burden and “pajama time”
The complexity of EHR also makes clinicians feel that they do more “button clicking” than engaging in conversations with patients. Burnout risk due to after-hours documentation, often called “pajama time,” is a documented consequence of poorly implemented EMR systems.
This disadvantage is real but not universal. Practices with well-designed templates, voice recognition, and ambient AI documentation tools report significantly lower documentation burden than those using default interfaces. The system’s usability and the practice’s investment in optimization make a substantial difference.
5. Security risk: centralization creates a high-value target
Paper records are vulnerable to physical damage (fire, flood) and localized theft. EMR systems are vulnerable to cyberattacks at scale. The average healthcare data breach cost $9.8 million in 2024 – nearly double the average across all other industries.
The risk of potential security and privacy-related challenges is always present. All providers need to take adequate measures to protect patient information, both in-transit and at-rest.
This does not mean EMRs are less secure than paper – a well-implemented EMR with proper security controls is significantly more resilient than filing cabinets. It means security must be treated as a core requirement, not an add-on, and vendor security certifications (SOC 2 Type II, HITRUST) must be verified rather than assumed.
6. Interoperability gaps between systems
53% of healthcare providers report facing challenges with EHR interoperability, leading to difficulties in exchanging patient information. Interoperability gaps contribute to patient safety issues, with 1 in 5 adverse events linked to incomplete information transfer between systems.
HL7 FHIR is the current standard for interoperability, but claiming FHIR compliance and actually achieving clean data exchange are different things. Implementation differences between vendors mean that even two FHIR-compliant systems may not exchange data reliably without custom integration work.
7. Vendor lock-in and data portability
EMR systems store data in formats that are often proprietary or difficult to export cleanly. Switching vendors after years of data accumulation is technically complex and expensive. Some vendors make migration deliberately difficult to prevent churn.
Before signing any EMR contract, verify that you can export your complete patient data in a standard format (HL7 FHIR, CSV, or equivalent) and test the export process before committing. A vendor who resists demonstrating data portability is signaling something important.
8. Ongoing maintenance and upgrade costs
Difficulty keeping up with frequent system upgrades and software changes is a commonly cited operational challenge, particularly for small practices without dedicated IT staff. Security patches, regulatory compliance updates (new ICD versions, billing rule changes, local MOH requirement updates), and feature upgrades all require ongoing attention and sometimes significant cost.
Cloud-based systems handle infrastructure maintenance on the vendor side, which reduces this burden substantially. On-premise installations carry the full maintenance load internally.
Electronic medical records for small practices
Small practices face a different cost-benefit equation than large hospital systems. The same EMR that delivers rapid ROI for a 300-bed hospital may not do so for a 3-physician family practice.
Specific advantages for small practices
Lower administrative overhead: A small practice that previously employed a full-time records staff member may find that EMR enables the same function with less dedicated staffing – or that existing staff can handle a larger patient volume without additional hires.
Billing accuracy: Coding assistance and automated claim submission reduce the billing errors that are disproportionately costly for small practices without dedicated coding staff. A single denied claim that would be easily caught in a large billing department can take a solo practitioner hours to resolve.
Telehealth integration: Cloud-based EMRs fully support remote patient monitoring and telehealth, enabling small practices to extend their reach without additional physical infrastructure. For solo practitioners or small rural practices, this is a meaningful competitive advantage.
Competitive parity: Patients increasingly expect online scheduling, patient portals, and e-prescriptions. Small practices without these capabilities face competitive disadvantage against larger systems that offer them as standard.
Specific disadvantages for small practices
Implementation cost relative to revenue: While EHR adoption is increasing, there are still challenges – like the cost of implementation and potential security concerns – for smaller organizations in particular. A $30,000 implementation cost represents a very different proportion of annual revenue for a solo practice than for a multi-physician group.
Limited IT support: Small practices typically lack dedicated IT staff to handle configuration, troubleshooting, and upgrades. This makes vendor selection more consequential: a vendor with poor support or a system that requires extensive IT maintenance is a worse fit for a small practice than for a large hospital with an IT department.
Workflow disruption: In a small practice, every provider is essential. A productivity dip during implementation affects patient throughput immediately and visibly – there is no slack in the system to absorb it the way a large organization can.
What small practices should prioritize in EMR selection
Cloud-based over on-premise: Eliminates infrastructure investment and places maintenance responsibility on the vendor.
Strong vendor support: Small practices need responsive support, not just documentation. Verify support response times and availability before committing.
Simplicity over feature depth: A system with fewer features that staff actually use is more valuable than a comprehensive system with a steep learning curve.
Transparent total cost of ownership: Get a full 3-year cost estimate including implementation, training, support, and any per-feature charges before comparing vendors.
Is an EMR worth it? A decision framework
The answer depends on your baseline, your goals, and your timeline.
EMR delivers the strongest ROI when:
- Your current billing error or claim denial rate is above 5%
- Your clinical staff spend more than 2 hours per day on documentation and administrative tasks
- Your practice is growing and manual record management is becoming a bottleneck
- You are participating or planning to participate in value-based care programs that require quality reporting
- Regulatory requirements in your market mandate digital records (PhilHealth eClaims in the Philippines, DOH EMR standards, etc.)
EMR delivers weaker ROI when:
- Your practice is very small (1-2 providers) with low administrative volume
- Your patient population has low turnover and paper records are manageable
- You are close to retirement or planning to close the practice
- Your workflows are highly non-standard and no available OTS system matches them without extensive customization
The honest middle ground: Most practices that implement a well-chosen EMR with proper planning and training see positive ROI within 2-4 years. The practices that see negative outcomes typically either chose a system that did not fit their workflows, underinvested in implementation, or failed to manage the change management process. The disadvantages listed above are real – but most are manageable with the right approach.
Build your EMR with Synodus
If you have concluded that a standard off-the-shelf EMR does not fit your workflows or compliance requirements, a custom or hybrid approach may deliver better long-term value.
Synodus is a Vietnam-based healthcare software development company with 250+ developers and 30+ healthcare implementations across APAC. Their hybrid model starts from a validated EMR base and extends it with custom modules for your specific workflows, local compliance requirements (Vietnam MOH, Philippine DOH/PhilHealth, Malaysian PDPA), and integrations.
Multi-field hospital complex: 700 beds, 2,500 outpatients and 800 staff daily. Custom EMR with cloud-based patient records, customizable templates, two-layer encryption, e-prescription, document scanning, and full integration with HIS, scheduling, and inventory management. Built in 4 months. Results: 70% improvement in operational efficiency, 90% decrease in incident rates, 3x faster diagnosis and treatment decisions, 85% of patient documents digitalized, under 3 seconds to create a digital medical record. Read the full EMR/EHR case study.
Vietnam University Hospital: 5,000 outpatients and 1,700 medical staff daily. Integrated EMR, inventory management, analytics dashboard, and patient mobile app. Results: 300% revenue increase, $70,000/month in administrative cost savings, 0.01% insurance claim denial rate.
BD Hospital: Major provincial general hospital serving 2,000+ outpatients daily. Implemented a web-based EMR on existing infrastructure with zero downtime during a facility transition. Results: zero system downtime, instant patient history access for all clinical staff, significant hardware cost savings.
Projects start within 48 hours of scoping completion
FAQs
The five most consistently documented advantages are: reduction in medication errors (30-38% in well-implemented systems), time savings for clinical staff (approximately 75 minutes per provider per day post-adaptation), faster and more reliable record access, improved preventive care and chronic disease management rates, and revenue cycle improvement through automated billing and coding. All five are contingent on implementation quality – a poorly implemented EMR delivers few of these benefits.
From a patient perspective, the primary disadvantages are: risk to data privacy in the event of a security breach, potential for documentation errors that persist in the electronic record and propagate across systems, and reduced face-to-face time with providers who are focused on screen documentation during visits. Interoperability gaps – where records cannot be transferred reliably between systems – also create care continuity problems for patients who see multiple providers on different platforms.
For most small practices, yes – but the timeline to positive ROI is longer and the selection process matters more. Cloud-based SaaS products at $200-$500/month minimize upfront costs. The key risks for small practices are implementation disruption (productivity dip during transition), ongoing maintenance without IT staff, and vendor lock-in. Prioritizing a cloud-based system with strong support, simple interface, and transparent total cost of ownership reduces these risks substantially.
The terms are often used interchangeably but the distinction matters for evaluating specific benefits. EMR advantages are primarily within-practice: better documentation, error reduction, billing automation. EHR advantages extend beyond the practice: cross-provider data sharing, care coordination across settings, patient engagement through portals, and population health analytics at scale. Most modern systems marketed as EMRs include many EHR capabilities. See the EMR vs EHR comparison for a detailed breakdown.
Revenue cycle improvements typically appear within 6-12 months. Clinical staff time savings reach full effect after 4-8 weeks of adaptation. Patient safety improvements from medication error reduction are measurable almost immediately post go-live. Full financial ROI, accounting for implementation costs, typically takes 2-4 years. Small practices should expect the longer end of this range.
The disadvantages listed above are real but not fixed – they scale significantly with implementation quality. Alert fatigue is worse when systems are deployed with default settings and never calibrated. Documentation burden is worse when templates are poorly designed. Vendor lock-in is worse when data portability was not verified before signing. Security risk is worse when vendors are not asked for third-party audit documentation. Most of the disadvantages cited in research on EMR problems trace back to implementation and selection decisions, not inherent limitations of digital records.





