What are electronic health records (EHR)?
An Electronic Health Record (EHR) is a comprehensive digital platform that collects, stores, manages, and exchanges patient health information across multiple healthcare settings. Unlike paper charts, EHRs make patient information available in real time to authorized providers regardless of where care is delivered: from primary care to specialist visits, emergency departments, laboratories, and pharmacies.
EHR systems serve as the central data infrastructure for modern healthcare delivery. They capture clinical data (diagnoses, medications, lab results, imaging), administrative data (demographics, insurance, appointments), and financial data (billing, claims, revenue cycle) in a single platform accessible across an organization.
According to the Office of the National Coordinator for Health IT (ONC), nearly 96% of non-federal acute care hospitals and 85% of office-based physicians in the United States have adopted certified EHR systems. The global EHR market was valued at $36 billion in 2024 and is projected to reach $93 billion by 2035, growing at 8.6% CAGR.
Despite near-universal adoption, challenges remain. Only approximately 30% of healthcare providers have achieved full EHR interoperability, meaning most organizations have digitized their records but have not yet unlocked the coordination benefits that EHRs are designed to deliver.
EHRs are one layer within a broader hospital information system (HIS). The HIS integrates EHR with administrative, financial, pharmacy, inventory, and operational functions across an entire facility. Understanding this distinction matters when scoping a digitalization project.
History of EHR
Understanding how EHR regulation evolved explains why systems are designed the way they are today, and why certain compliance requirements exist that would otherwise seem arbitrary.
1996: HIPAA establishes the baseline. The Health Insurance Portability and Accountability Act created the first federal standards for protecting patient health information electronically. HIPAA’s Security Rule and Privacy Rule are still the foundation of EHR compliance in the US, defining the minimum requirements for encryption, access controls, audit logging, and breach notification that every system must meet.
2009: HITECH creates the financial incentive for mass adoption. The Health Information Technology for Economic and Clinical Health Act allocated over $27 billion to encourage healthcare providers to adopt certified EHR systems and demonstrate “meaningful use” of those systems through Medicare and Medicaid incentive payments. This is the primary reason US hospital adoption went from under 10% in 2008 to 96% by the mid-2010s. It also created the ONC certification framework that vendors must still meet today.
2011-2015: Meaningful Use stages define what EHRs must do. The three-stage Meaningful Use program, later renamed Promoting Interoperability, progressively raised the bar for what certified EHRs were required to support: e-prescribing, patient portals, clinical decision support, care summary exchange, and eventually population health reporting. These stages are why modern EHRs include patient portals and CDS as standard features rather than add-ons.
2016: 21st Century Cures Act targets information blocking. Despite widespread EHR adoption, data was still not flowing freely between systems. The 21st Century Cures Act prohibited “information blocking” by EHR vendors, health systems, and health IT networks, requiring that patient data be shareable through open, standardized APIs. This legislation is the legal foundation for FHIR API mandates and the reason EHR vendors can no longer restrict patient data access without significant penalty.
2020-2025: FHIR becomes the interoperability standard. Following the 21st Century Cures Act, ONC and CMS issued rules requiring certified EHR systems to support HL7 FHIR R4 APIs for patient data access. By 2024, USCDI v3 compliance had become the federal benchmark for data exchange. Epic adopted USCDI v3 standards ahead of the December 2025 deadline, signaling broad industry alignment. This is why “FHIR support” is now a minimum requirement rather than a differentiating feature when evaluating EHR vendors.
The implication for procurement today: EHR features and compliance requirements did not emerge from vendor innovation alone. They were largely mandated through successive waves of regulation. When evaluating systems, this history explains why certain capabilities exist across all certified products, and where genuine differentiation between vendors actually lies.
EHR vs EMR: Understanding the difference
The terms are often used interchangeably, but the distinction is operationally significant.
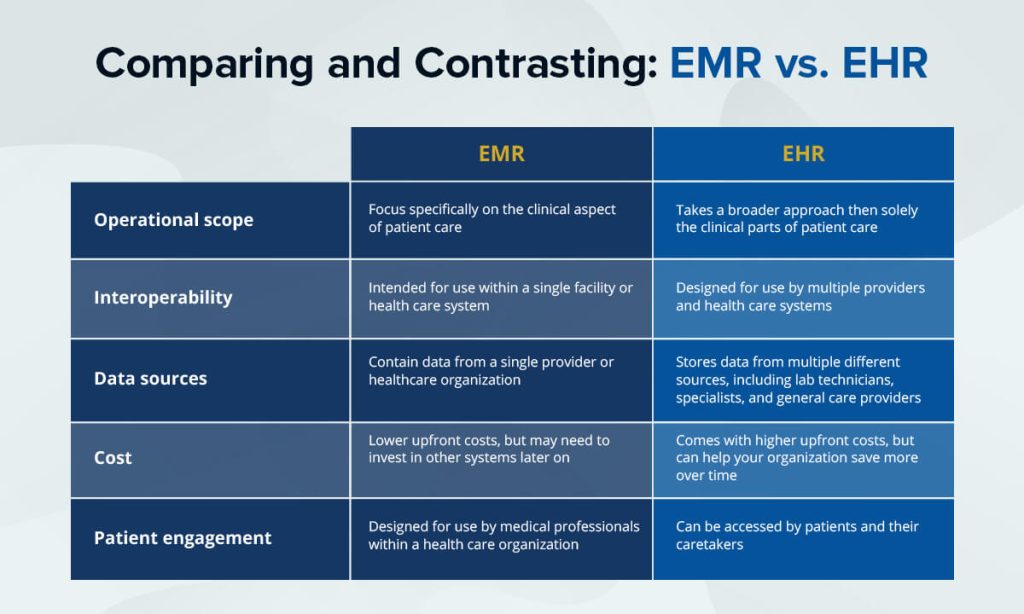
An EMR (Electronic Medical Record) is a digital version of a patient’s chart within a single practice or facility. It stores clinical data for use by that organization’s own providers. Data does not automatically travel with the patient to other care settings.
An EHR is designed to share information across multiple providers and care settings. A patient’s EHR follows them from their primary care physician to a specialist, from an urgent care clinic to a hospital emergency department. It is built for longitudinal, coordinated care rather than episodic, single-provider documentation.
The practical difference: when a patient arrives at a hospital emergency department, an EMR-only environment means the emergency physician has no visibility into the patient’s medications, allergies, or recent lab results unless the patient can recall them. An EHR environment means that information is accessible immediately, reducing errors and duplicate testing.
For a full breakdown of how EMR, EHR, and PHR differ, see the EMR vs EHR vs PHR comparison guide. For a deep dive into EMR specifically, see the complete EMR guide.
Core features of a modern EHR system
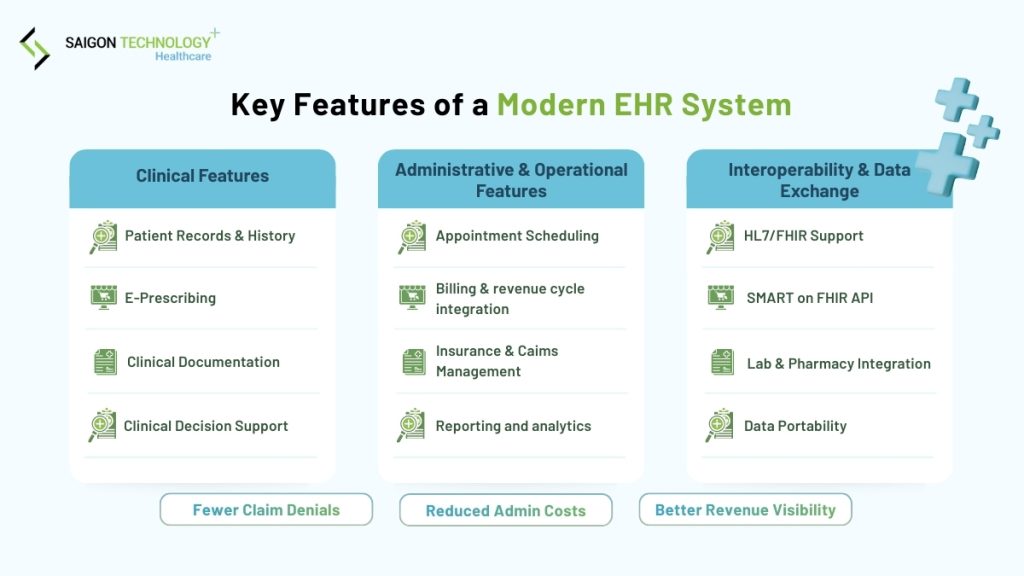
Contemporary EHR platforms integrate dozens of capabilities. These are the ones that determine whether a system actually improves care delivery.
Patient management and registration
The foundation of any EHR. Patient management covers demographic information, insurance details, emergency contacts, and preferences. Modern systems include patient portals for online scheduling, test result access, secure messaging, prescription refill requests, and bill payment. Patient portals reduce administrative phone volume and improve engagement with preventive care.
Advanced patient management includes automated appointment reminders, waitlist management, and patient education material distribution. Accurate record matching across visits prevents duplicate records, which is a significant patient safety risk at high-volume facilities.
Clinical documentation
Clinical documentation enables providers to record patient encounters, create progress notes, document diagnoses, and develop treatment plans. Modern EHRs offer customizable templates, voice recognition for dictation, structured data entry, and smart phrase libraries that reduce repetitive typing.
The best systems balance structured data capture with narrative flexibility. Templates should guide documentation without forcing providers into rigid workflows that slow them down or produce notes that look templated rather than clinically meaningful.
Electronic prescribing and medication management
E-prescribing transmits prescriptions directly to pharmacies electronically, checks drug-drug interactions and allergies in real time, and integrates with prescription drug monitoring programs (PDMPs) to flag controlled substance risks.
Medication management tracks the full medication list, flags discrepancies during care transitions (medication reconciliation), and supports formulary checks to guide cost-effective prescribing. This is one of the highest-impact features for patient safety: a Carnegie Mellon study linked full EHR adoption to approximately a 30% reduction in prescription errors.
Laboratory and diagnostic integration
EHR integration with laboratory information systems (LIS) and radiology systems (RIS/PACS) enables electronic test ordering, automatic result delivery, and image viewing within the EHR interface. Abnormal results trigger provider notifications. Results trend over time, making it easy to identify patterns rather than reviewing each result in isolation.
This integration eliminates manual transcription of lab results, which is a common source of data entry errors in facilities that lack it.
Clinical decision support
Clinical decision support (CDS) delivers real-time alerts and guidance at the point of care: drug interaction warnings, allergy checking, preventive care reminders, diagnosis-specific order suggestions, and evidence-based clinical guidelines.
CDS is powerful when well-configured and counterproductive when poorly configured. Overly aggressive alerting creates alert fatigue, where providers begin ignoring alerts reflexively, including the ones that matter. Research published in JAMIA found 93% override rates for drug interaction alerts in systems with high alert volumes. A separate study in the Journal of General Internal Medicine found acceptance rates for the most severe alerts fell from 100% to 8.4% after switching to a commercial EHR that generated six times more alerts. Configuring CDS thresholds carefully is one of the most important implementation decisions an organization makes.
Billing and revenue cycle management
Integrated billing connects clinical documentation directly to charge capture, claims submission, and payment processing. Automated charge posting based on documentation reduces missed charges. Claims scrubbing identifies errors before submission, reducing denial rates. Electronic remittance processing and patient statement generation streamline collections.
Revenue cycle integration is typically where EHR ROI is most quickly visible. Organizations routinely report improved coding accuracy and faster claim processing within the first year of full implementation.
Reporting and population health analytics
EHR reporting tools support quality metric monitoring, clinical outcome tracking, operational efficiency analysis, and regulatory reporting for programs like MIPS and HEDIS. Population health dashboards aggregate data across patient panels to identify care gaps, track chronic disease control, and stratify risk.
These capabilities become increasingly important as healthcare moves toward value-based reimbursement models that reward quality and outcomes rather than volume.
Key benefits – With real data
Medication error reduction. A study in npj Digital Medicine (Nature, 2023) found a 38% reduction in voluntarily reported medication incidents after transitioning from paper to digital records, with prescribing errors falling from 52.8% to 15.7% of orders reviewed. Healthcare institutions using EHR data analytics report a 40% decrease in diagnostic errors compared to paper-based systems.
Time savings. Research published in PubMed Central found savings of around 75 minutes per provider per day once clinical staff fully adapted to the EHR system. EHR adoption also cuts time spent on insurance eligibility tasks by more than 80% according to proponents cited in a Wikipedia review of EHR research.
Revenue improvement. Healthcare organizations with advanced EHR data integration report an average 25% increase in annual revenue through better identification and optimization of care gaps and revenue opportunities.
Preventive care rates. EHR alerts and reminders raise screening and vaccination rates by 10-20% compared to paper-based systems, particularly for chronic disease management and age-appropriate screenings.
Cost of inaction. The average cost of a healthcare data breach reached $9.8 million per incident in 2024. Facilities without digital records and proper security infrastructure face compounding risks from paper-based record keeping, manual processes, and the difficulty of demonstrating compliance during audits.
For a detailed cost and ROI breakdown, see the EHR cost and ROI guide.
Types of EHR systems
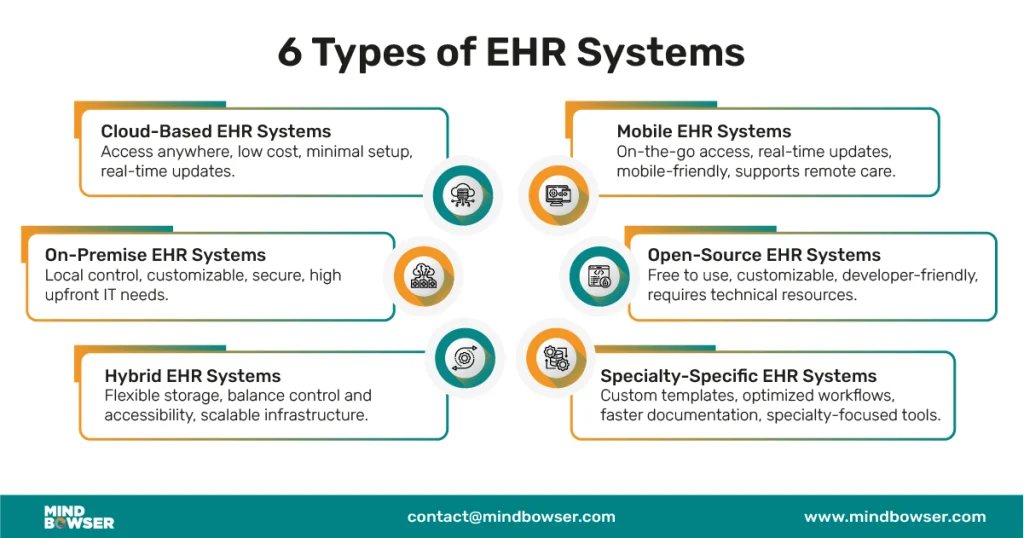
By deployment model
Cloud-based EHR stores data on vendor-managed servers, accessed via browser or mobile app. Low upfront investment, automatic updates, and accessible from any device. Requires stable internet connectivity. The default choice for most new implementations: 83.4% of EHR systems are cloud or web-based as of 2024.
On-premise EHR installs on the organization’s own servers. Full data control, no internet dependency for core functions, better suited to data sovereignty requirements. Requires dedicated IT staff and capital investment for infrastructure and refresh cycles.
Hybrid combines both: core clinical data on-site, patient portals and analytics in the cloud. Increasingly common for mid-to-large hospitals balancing reliability, compliance, and remote access requirements.
By facility type
Inpatient EHR is designed for hospital settings with a focus on cross-department interoperability: admissions, nursing, pharmacy, laboratory, radiology, and billing all working from a shared record. Bed management, order sets, and nursing documentation workflows are core.
Outpatient/ambulatory EHR serves clinics and physician practices. Appointment scheduling, encounter documentation, e-prescribing, and billing are the primary workflows. Less focused on bed management and more focused on patient visit throughput.
Specialty-specific EHR is tailored to the documentation and workflow needs of a specific clinical discipline: mental health (BIRP notes, treatment plan tracking), oncology (chemotherapy protocols, cycle management), ophthalmology (visual acuity, imaging integration), dentistry (odontogram, periodontal charting). If your specialty has genuinely distinct documentation requirements, a specialty system covers them out of the box; a general EHR requires significant customization to match.
Interoperability: Why it determines whether your EHR actually works
Interoperability is the ability of EHR systems to exchange and use data from other systems. It is the feature that separates an EHR from an EMR in practice, not just in definition.
The data on where interoperability stands is sobering. 70% of US hospitals use EHR systems from different vendors, creating persistent compatibility gaps. Only 30% of providers have achieved full interoperability. Physicians in a 2024 KLAS Arch Collaborative survey cited interoperability as their top fix request, noting that external patient data is often unavailable in their EHR and, when found, difficult to use clinically.
The consequence is real: 52% of physicians report delays in patient care due to difficulty accessing data from external EHR systems.
The standards that matter
HL7 FHIR (Fast Healthcare Interoperability Resources) is the current standard for EHR data exchange. FHIR uses modern web APIs to enable flexible, scalable data sharing between systems. US federal regulations now mandate FHIR support for patient data access. Any EHR evaluated today should support FHIR R4 as a minimum.
HL7 v2 remains widely used for specific high-volume interfaces: laboratory result delivery, admission-discharge-transfer (ADT) notifications, and pharmacy messages. Many EHR systems support both v2 and FHIR simultaneously.
DICOM is the standard for medical imaging data. If your facility produces or receives imaging (X-ray, MRI, CT, ultrasound), verify that your EHR integrates with PACS using DICOM.
USCDI (United States Core Data for Interoperability) defines the minimum dataset US EHRs must be able to exchange. As of late 2025, USCDI v3 compliance is the regulatory benchmark.
What to verify before signing a contract
Do not accept “HL7 compliant” as sufficient. Ask which version of FHIR the system supports, whether they have live integrations with the specific external systems you need to connect (reference labs, imaging centers, regional health information exchanges), and whether those integrations are included in the base contract or priced separately.
Compliance standards every EHR must meet
HIPAA
The Health Insurance Portability and Accountability Act establishes the minimum security and privacy standards for any system storing US patient data. Technical safeguards include access controls, audit logging, automatic logoff, encryption at rest and in transit, and transmission security. Administrative safeguards require risk assessments, workforce training, and incident response procedures.
Ask any EHR vendor for their most recent HIPAA risk assessment and third-party audit documentation. “We are HIPAA compliant” is not verifiable without documentation.
ONC certification
The Office of the National Coordinator for Health IT certifies EHR systems that meet federal standards for patient data access, interoperability, and clinical quality reporting. ONC certification is required to participate in certain government programs including MIPS and Promoting Interoperability.
FHIR API requirements
As of 2025, US regulations require certified EHR systems to provide open, standardized FHIR APIs that allow patients to access their health data through third-party applications of their choice. This is part of the 21st Century Cures Act’s information blocking provisions. EHRs that restrict patient data access can face significant penalties.
GDPR
For organizations serving patients in the European Union or handling EU citizen data, GDPR grants individuals rights to access, correct, delete, and port their personal data. EHR systems must implement consent management, data subject request workflows, and automated retention policies.
Local regulatory requirements
Outside the US and EU, local health ministries and MOH bodies impose their own standards. In Southeast Asia: Vietnam MOH regulations, PhilHealth and DOH requirements in the Philippines, PDPA in Thailand, MOH Malaysia standards. In Australia: TGA and Australian Privacy Act. Verify that your vendor has actually deployed in your specific regulatory environment, not just in markets with similar-sounding regulations.
Build vs buy: How to decide
This is one of the most consequential decisions in EHR procurement, and the one most organizations make without enough context.
When off-the-shelf makes sense
OTS EHR systems are the right starting point for most organizations. They represent decades of development investment incorporating best practices from thousands of implementations, carry existing regulatory certifications, come with vendor-provided training and support, and deploy in 3-12 months rather than 12-24 months for custom builds.
OTS works well when your workflows are standard, your compliance requirements are met by the vendor’s existing certifications, and your facility does not have deeply specialized clinical workflows that a general system cannot accommodate.
When custom or hybrid makes sense
Custom development becomes the better long-term investment when your facility operates at high volume with complex multi-department workflows, needs to comply with local regulations that international OTS products are not built for, has specialty clinical workflows that require extensive customization of any OTS system, or is scaling across multiple facilities with varying configurations.
The hybrid approach (validated base system plus targeted custom development) is increasingly the preferred path for mid-to-large hospitals. It compresses deployment timelines relative to full custom builds while preserving flexibility that pure OTS cannot offer. A useful test: if you find yourself saying “but we do it differently” more than twice during a vendor demo, you likely need custom or hybrid.
For a real example of how the hybrid approach plays out, the Synodus EHR case study for a multi-field hospital complex documents the full decision-making process: why the client ruled out OTS, how a packaged base was extended with custom modules, and measurable outcomes after go-live.
Comparison at a glance
| Factor | Off-the-shelf | Custom / hybrid |
|---|---|---|
| Implementation time | 3-12 months | 12-24+ months |
| Upfront cost | $15,000-$70,000 per provider | $250,000-$2M+ |
| Ongoing costs | 18-25% of license annually | 15-20% of build cost annually |
| Customization | Limited to configuration | Fully flexible |
| Compliance | Pre-certified for major markets | Built to your regulatory environment |
| Vendor dependency | High | Low |
| Long-term fit | May require replacement at scale | Adapts as you grow |
Cost breakdown and ROI
What EHR implementation actually costs
Software licensing (OTS): $500-$2,000 per user for the initial license, plus 18-25% of license cost annually for support and updates. SaaS subscriptions typically run $200-$1,200 per provider per month.
Custom development: $100-$200+ per hour for experienced healthcare software development teams. A basic EHR for a small practice requires 3,000-5,000 development hours ($300,000-$1M). A comprehensive hospital system can require 15,000-30,000+ hours ($1.5M-$6M+).
Implementation services: Configuration, data migration, interface development, training, and go-live support typically add 30-50% on top of license or development costs. A 2025 analysis estimated average implementation support costs at approximately $6,200 per user, meaning a 100-user deployment carries $620,000 in implementation costs before the license fee.
Infrastructure: Cloud deployments run $2,000-$10,000+ monthly depending on size. On-premise requires $50,000-$500,000+ in server hardware, plus IT staffing.
Compliance and certification: HIPAA assessments and security audits run $15,000-$50,000 annually. ONC certification for custom systems costs $25,000-$100,000.
Training: Budget $200-$500 per user for comprehensive training programs.
ROI timeline
EHR investments rarely deliver immediate ROI. The first 12-18 months typically involve net costs as implementation expenses are incurred and productivity temporarily decreases during transition. Break-even typically occurs 2-3 years post-implementation.
Long-term ROI comes from efficiency gains (5-15% productivity improvement), revenue capture improvements (2-5% from better coding and charge capture), cost reductions (transcription, storage, administrative overtime), and quality improvements (fewer errors, better preventive care rates).
For a detailed cost breakdown by deployment model and facility size, see the EHR cost and ROI guide.
Common challenges and how to handle them
User adoption resistance
Clinical staff, particularly physicians with established workflows, frequently resist new EHR systems. Root causes include perceived productivity loss, skepticism about benefits, and lack of involvement in system selection. Organizations with strong stakeholder engagement achieve significantly higher adoption rates within six months of go-live.
Mitigation: involve frontline clinicians in workflow design before the system is configured. Identify physician champions early. Invest in role-specific training, not generic sessions. Provide intensive go-live support for the first 30-60 days. See the EHR implementation challenges guide for specific strategies.
Data migration
83% of data migration projects either fail or exceed their budgets and timelines (Gartner). In healthcare, migration failure is a patient safety risk: incomplete or corrupted records create clinical decision gaps.
Mitigation: treat migration as a separate workstream with its own lead and budget. Audit source data before migration begins. Map every field from legacy to new system. Validate migrated data before go-live. Build in a parallel-running period to catch missed records.
Interoperability gaps
Even when two systems are both HL7 FHIR compliant, real-world data exchange can still fail due to implementation differences, data model variations, and vendor decisions that limit portability.
Mitigation: before signing any contract, map every external system you need to connect with and verify the vendor has a live integration with each one. Ask for a reference from a customer using that specific integration.
Alert fatigue
Poorly configured clinical decision support generates too many alerts, training clinicians to click through without reading. Studies show override rates of 90%+ in high-alert-volume systems, including overrides of clinically significant warnings.
Mitigation: configure alert thresholds carefully during implementation. Disable or downgrade low-severity alerts. Review override patterns quarterly and reconfigure alerts with high override rates.
How to choose the right EHR
Start with these four questions before evaluating any specific product.
1. What is your facility type and patient volume? A 20-provider ambulatory clinic and a 400-bed hospital have fundamentally different requirements. Large inpatient facilities need cross-department interoperability, bed management, and order set capabilities that ambulatory-focused systems do not prioritize. Make sure you are evaluating systems designed for your care setting.
2. What are your specific compliance requirements? US facilities need HIPAA compliance and ONC certification. European facilities need GDPR capabilities. Southeast Asian hospitals need local MOH standard compliance, which most international OTS products are not built for. Verify compliance fit before shortlisting vendors, not during negotiation.
3. OTS, custom, or hybrid? If your workflows are standard and your compliance requirements are met by existing certifications, OTS is faster and cheaper upfront. If you have complex workflows, local regulatory requirements not covered by OTS products, or are scaling across multiple facilities with different configurations, custom or hybrid delivers better long-term ROI despite higher initial investment.
4. Standalone EHR or part of a broader HIS? If you are digitizing a hospital rather than a single clinic, buying a standalone EHR and integrating it later with billing, inventory, and pharmacy adds significant technical debt. Scoping an HIS that includes EHR as a module means integrations are built in from the start. For guidance on evaluating vendors for hospital-wide implementations, see the HIS companies evaluation guide.
Once these decisions are made, evaluate shortlisted vendors using structured scoring across six criteria: compliance verification (documented, not claimed), interoperability (live integrations with your specific external systems), implementation track record at comparable facilities, five-year total cost of ownership, scalability and roadmap, and long-term support model.
Frequently Asked Questions (FAQ)
OTS SaaS products typically run $200-$1,200 per provider per month. Enterprise licensing ranges from $15,000-$70,000 per provider upfront, plus 18-25% annually for support. Custom development starts at $300,000+ for smaller builds and scales significantly for large hospital systems. Implementation costs (configuration, migration, training, go-live support) add 30-50% on top. For a full breakdown, see the EHR cost guide.
Small ambulatory practices implementing OTS systems: 3-6 months. Mid-size hospitals: 12-18 months. Large health systems or custom builds: 18-30 months. Data migration is consistently the phase most organizations underestimate.
ONC certification is required to participate in government programs including MIPS and Promoting Interoperability. It is also increasingly expected by insurers and health system affiliates as a baseline quality indicator. For facilities outside the US, the equivalent is certification by the relevant national health IT authority (DOH, MOH, etc.).
Interoperability is the ability of EHR systems to exchange and use data from other systems. It is what makes an EHR function as a coordinated care tool rather than just a digital filing cabinet. Only 30% of healthcare providers have achieved full interoperability despite near-universal EHR adoption, meaning most organizations have digitized records but have not fully realized the coordination benefits EHRs are designed to deliver.
No. An EHR covers clinical records and care coordination. A hospital information system (HIS) integrates EHR with administrative, financial, pharmacy, inventory, HR, and operational functions across the entire facility. For hospital-wide digitalization, an HIS that includes EHR as a module is a more complete and cost-effective long-term architecture than a standalone EHR with point integrations built over time.
At minimum: HIPAA (US), ONC certification (US government programs), FHIR API requirements (21st Century Cures Act), GDPR (EU patient data). For local deployments: Vietnam MOH, Philippine DOH/PhilHealth, Thailand PDPA, Australia TGA and Privacy Act. Verify compliance fit for your specific market before shortlisting vendors. Ask for certification documentation, not self-reported claims.
User adoption failure. A technically sound system that clinical staff resist produces the same outcomes as no system at all. The evidence is clear: facilities that involve frontline clinicians in workflow design before configuration significantly outperform those that present the system to staff after it is already built. Invest in change management as seriously as you invest in the software itself.





